Just saw this. Not vaccine related, treatment related.
https://www.abc12.com/2020/11/20/st-...-19-treatment/



Just saw this. Not vaccine related, treatment related.
https://www.abc12.com/2020/11/20/st-...-19-treatment/
In the P-F basket of deplorables.

That's awesome.Originally Posted by Borderland

Sorta around sometimes for some of your shitty mod needs.

Hopefully true, but I swear every single week of this entire pandemic there's been an article about scientists somewhere making some great discovery about treatment/prevention of covid, and then you never hear of it again. I'm starting to wish they'd just shut up unless it's actually been proven at least well enough to get emergency use authorization.

It gets even better. The office she has to report to is closed on the weekend.
I'll wager you a PF dollar 😎
The lunatics are running the asylum

Meh. Ive heard it played much better. Intonation was slipshod, tempo was lugubrious, and the playing was at times jejeune, self-indulgent and capricious.


General rule here is to call the charge nurse and let them deal with it.
As far as exposure to unknown (in real time) risks itself, this a new reality. We've a first office personnel, a nurse care manager, coming down with it. Who knows how many coworkers were exposed, and that person didn't like wearing masks.
Doesn't read posts longer than two paragraphs.
Well, it worked for the mice.
In the P-F basket of deplorables.
As someone who tends to use up 40+ hours of sick leave after a flu shot, effective treatments are at least as interesting to me as the vaccines. Not an anti-vaxxer, it's just that the one that people tend to freak out over not getting has a lousy track record for me.
Meanwhile, when this first started, and having a solid case of the, "How can I help?"'s, I cranked up an old workstation and an older laptop and started Folding@home. It's a distributed computing project that works on covid, alzheimers, parkinson's, cancer, and huntington's. You set it up and it runs on your pc 24/7 if you like, or just when you aren't using it.
I'm currently at 90,229, 651 points, any meaning of which is beyond me other than it's more than yesterday. And monthly I've been near the top 3000 out of what looks to be 255,000 current contributors. Cytokines and an assortment of proteins seem to be what's being worked on by my pc (the laptop died) the most. So perhaps, I've helped in however dinky a way. And if not, that's still good news. Thanks for posting.

The paper itself (here) seems 'interesting' but it's still just a mouse model of infection. They've trialled a lot of anti-inflammatory cytokine targeted drugs (dexamethasone toculizumab plus a million other -mabs) and it seems like dexamethasone is modestly protective but the rest has yet to prove out.
As I've cautioned before, the pathophysiology of critical illness (which includes severe COVID-19) is incredibly complex and poorly understood. Even more challenging is that the most severe presentation of many different disease processes (including bacterial sepsis, trauma, pancreatitis, and of course severe COVID-19, to name a few) end up culminating in nearly identical clinical syndromes (eg ARDS), so "what" you are treating (and whether or your novel targeted therapeutic is the right tool for the job) is a fairly messy question.
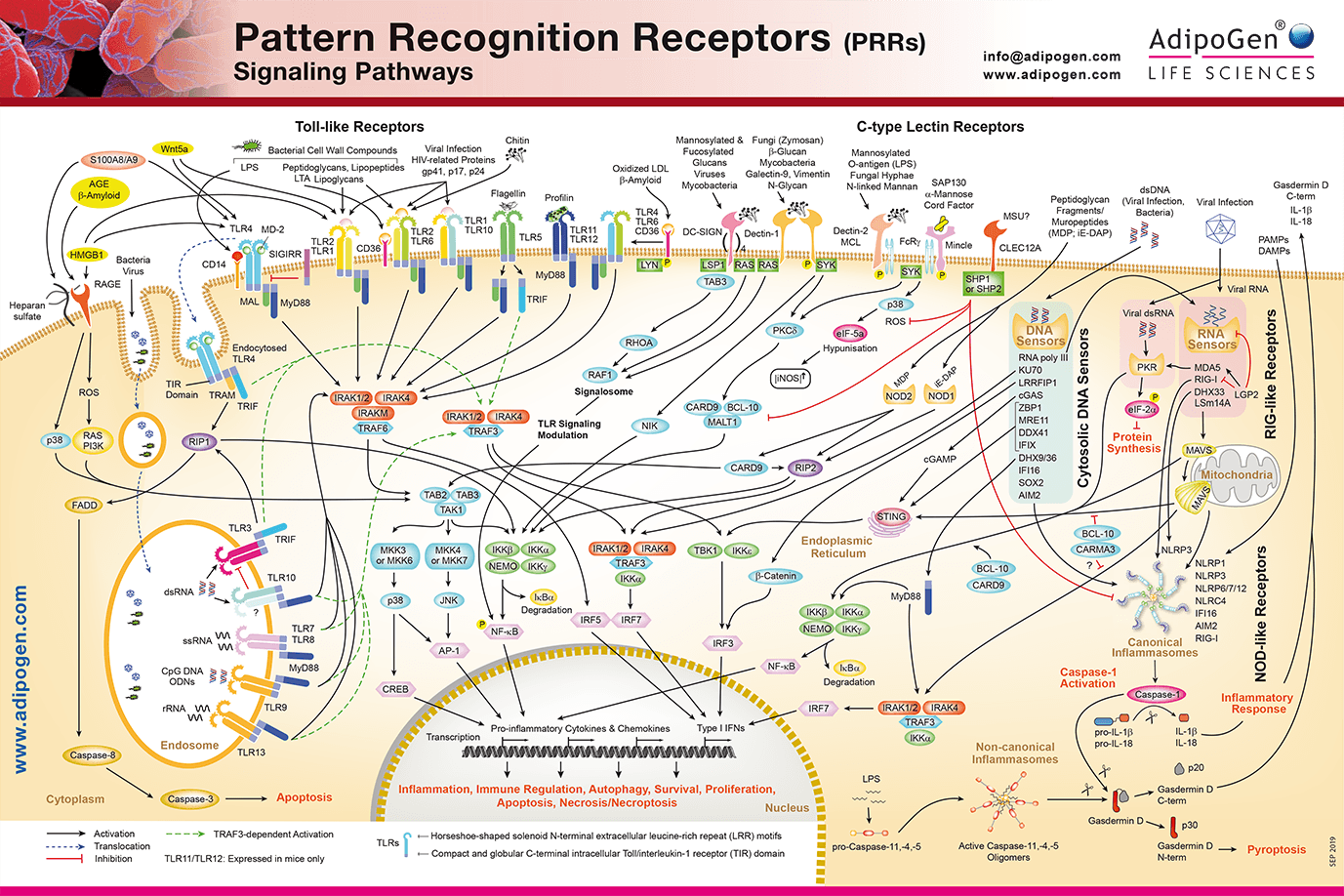
That's the problem with handwaving about "cytokine storms." Cytokines are just little signaling molecules that are released by one cell and change the behavior of the cells it reaches, and they interact in an insanely complicated network that we no doubt do not actually understand. To give you an idea of what I am talking about, here's cell signaling poster highlighting the extra/intracellular networks of PRRs, which are related to the "cytokine storm" phenomenon:
And that is just one signaling network out of hundreds...
So, for that reason, while occasionally we are able to find magic bullet medications (Gleevec is a reasonable example of this), in practice, it is extremely hard to dissect out a process as complex and nuanced as inflammatory signaling of critical illness and turn it into a drug that works to help real people.
...yeah, my head hurts just looking at the pictures. I know we aren't supposed to trust "experts" any more, I'm sure some laymen will sort it out.
Sorta around sometimes for some of your shitty mod needs.

 Reply With Quote
Reply With Quote